Porcelain Filling (Inlay or Onlay)
This article outlines the indications, diagnostic evaluation, procedural steps, risks, material considerations, and recovery expectations associated with porcelain inlays and onlays, supporting patients in making informed decisions with guidance from qualified dental professionals.
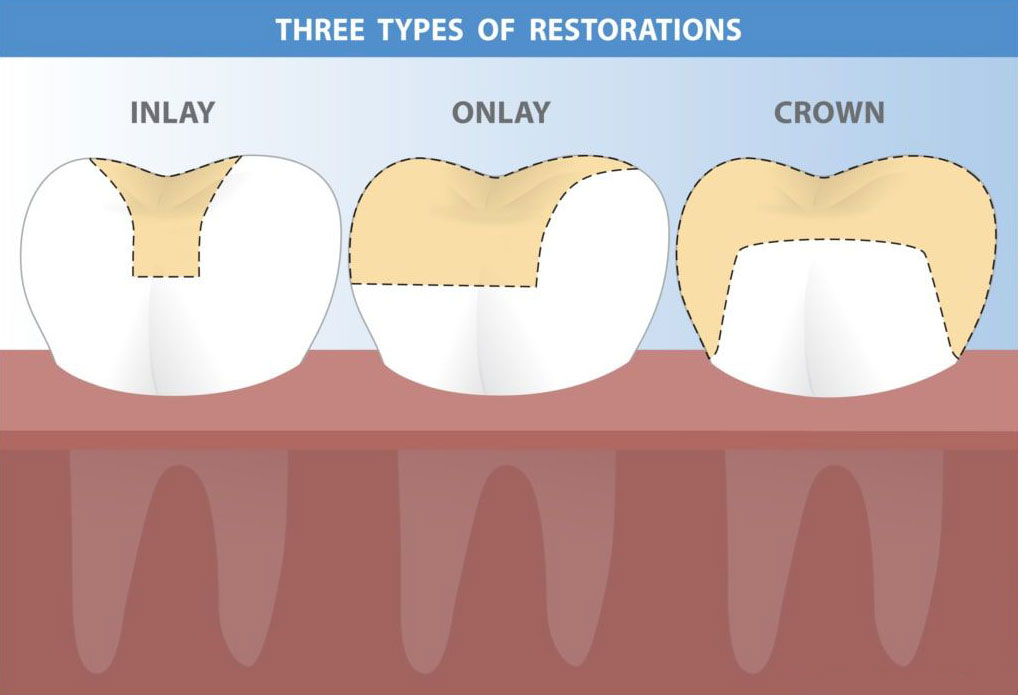
A porcelain filling, also known as a porcelain inlay or onlay, is an indirect dental restoration used to repair teeth affected by moderate decay, structural fractures, or loss of tooth integrity that does not yet require full crown coverage, and it is chosen when preserving as much natural tooth structure as possible is clinically appropriate. These restorations are manufactured from durable ceramic materials and are designed to fit precisely within or over a prepared tooth cavity, with inlays occupying the space between the tooth cusps and onlays extending over one or more cusps when additional support is needed. Patients may be evaluated for symptoms such as discomfort when chewing, increased tooth sensitivity, visible fractures, or recurrent decay around older fillings, and causes can include weakened enamel, long-standing dental caries, biting forces that exceed natural tooth strength, or failing composite or amalgam restorations. Diagnosis involves a comprehensive clinical examination, radiographic imaging to assess the extent of decay or crack propagation, and evaluation of the tooth’s structural soundness to determine whether a porcelain inlay or onlay is an appropriate restorative choice or whether a dental crown is needed instead. When indicated, porcelain inlays and onlays provide a conservative alternative to crowns by retaining healthy enamel and dentin while restoring functional anatomy and preventing further fracture. The procedure typically begins with local anesthesia, followed by careful removal of decayed or damaged tooth structure using minimally invasive restorative dentistry techniques designed to maintain maximum natural tissue. The dentist then shapes the tooth for optimal adaptation of the porcelain restoration and records the preparation using either traditional impression materials or digital scanning technologies. Digital CAD/CAM dentistry may allow for increased precision and streamlined fabrication, though some cases require laboratory processing, in which a temporary restoration protects the tooth while the final inlay or onlay is created. Once the porcelain restoration is ready, the clinician verifies its fit, contour, and occlusion before bonding it to the tooth using adhesive cement. The bonding process requires strict moisture control and involves treatment of both the tooth and ceramic surfaces, allowing for a durable bond that supports functional forces. After placement, the dentist adjusts the bite to ensure even distribution of occlusal pressure and polishes the restoration to create a smooth finish that blends with the natural tooth. Patients may experience temporary sensitivity to temperature or pressure due to changes in dentin exposure or adjustment to new bite contacts, but these symptoms typically diminish as the tooth adapts. Risks associated with porcelain fillings include fracture of the restoration under high biting stress, debonding if moisture control during placement is compromised, marginal leakage if decay develops at the interface, or postoperative sensitivity that occasionally requires further evaluation. These risks may be influenced by factors such as bruxism, inadequate oral hygiene, extensive preexisting enamel loss, or the location of the restoration in areas subject to heavy chewing forces. Despite these considerations, porcelain inlays and onlays offer several clinical advantages, including excellent fit, high biocompatibility, resistance to staining, and preservation of natural tooth structure, making them a preferred choice in many moderate-damage cases. Longevity depends on oral hygiene practices, routine dental evaluations, avoidance of excessive biting forces, management of underlying conditions such as clenching or grinding, and the quality of the bonding process. Patients often ask how long porcelain inlays or onlays last, and although outcomes vary, properly maintained restorations can function for many years due to the strength of modern ceramic materials. Recovery after placement is generally straightforward, with most individuals able to resume normal eating shortly after anesthesia wears off, though clinicians may recommend avoiding very hard foods temporarily to protect the new restoration. Postoperative care includes maintaining regular brushing and flossing, attending follow-up visits to monitor restoration integrity, and notifying a dental professional if symptoms such as persistent sensitivity, biting discomfort, or visible edge changes occur. Porcelain inlays and onlays can also enhance long-term oral health by reinforcing weakened teeth, reducing the risk of future cracks, and creating smooth surfaces that discourage plaque accumulation. When comparing porcelain fillings to other options such as composite fillings or full crowns, dentists consider factors including decay severity, remaining tooth structure, aesthetic goals, and functional demands, emphasizing that no single restoration is suitable for all cases. Understanding the purpose, diagnostic criteria, procedural sequence, benefits, limitations, and potential risks of porcelain inlays and onlays helps patients participate meaningfully in treatment planning. Ultimately, individuals should consult a qualified dental professional to determine whether a porcelain filling is appropriate based on their specific oral health condition and overall restorative needs, ensuring decisions are made safely and in alignment with evidence-based clinical standards.